TRT Reference Page
![]()
Needle lengths and my entire page on IM lengths
Lowering H&H and raising ferritin <--- IF YOU GOOGLED 'VORCK PROTOCOL' THIS IS WHAT YOU WANT
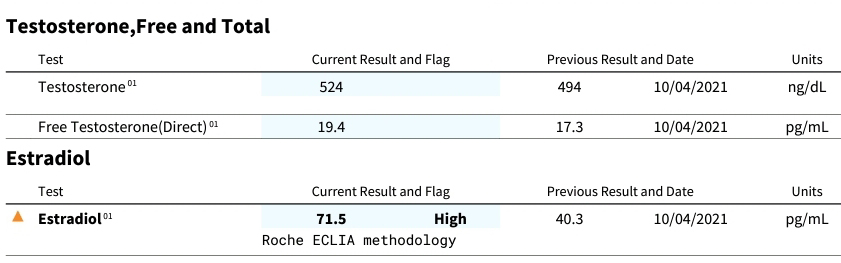
Labs to order before, during TRT
E2 and DHT predictor calculators based on Total Testosterone
Order your own labs (Discounted Labs)
Order your own labs (Doctor Says)
Any topic that is in a dropdown is optional reading for the curious. It's not really central to the main topics of high hemoglobin and hematocrit or building ferritin.
Abbreviations
TRT - Testosterone Replacement Therapy. The use of exogenous testosterone (or sometimes alternatives like hCG/SERMs) to restore testosterone levels and alleviate symptoms of deficiency.
AI - Aromatase Inhibitor. Aromatase is an enzyme that helps to make estrogen from Testosterone. An inhibitor slows down the production of this enzyme so that you make less estradiol. This class of drug does not "block estrogen."
BMI - body mass index, calculator 1 or calculator 2, explanation that BMI doesn't reflect health, alternate discussion of same
ED - Every Day (daily dosing/microdosing).
EOD - Every Other Day. Common frequency for more stable levels than once-weekly injections.
hCG - Human Chorionic Gonadotropin - discussion
IM - intramuscular
SC - subcutaneous, sometimes written SQ
E2 or Estradiol - The primary estrogen in men. Measured in pg/mL. Important to monitor on TRT as testosterone can aromatize into it.
LH - Luteinizing Hormone. Pituitary signal that tells the testes to produce testosterone. Suppressed on exogenous TRT.
FSH - Follicle-Stimulating Hormone. Works with LH on testicular function and spermatogenesis. Also suppressed on standard TRT.
SHBG -
Testosterone and Estradiol are predominately bound to this plasma protein, and the Testosterone unbinds and enters cells expressing megalin. Steroids not bound to SHBG may bind to Albumin or may circulate as Free Testosterone or Free Estradiol. SHBG does not inactivate Testosterone. This has been known for 20 years.
TT - Total Testosterone. Please don't make people crazy, use ng/dL
FT - Free Testosterone. Please use pg/mL
Needle sizes
TAP TO OPEN LARGER ON MOBILE, OR
RIGHT CLICK, "OPEN IN NEW WINDOW" ON DESKTOP

[Source of graphic]
The Vorck Needle Length Page showing length needed for IM injections based on BMI
Labs to get
Get before and occasionally after starting TRT:
• Total Testosterone
• Free Testosterone
• SHBG (Albumin is a common one docs also add in addition to SHBG)
• Estradiol (specify "sensitive assay for males")
• Prolactin
• Progesterone (for women, this isn't necessary for men)
• PSA
• Vitamin D
• Ferritin (an iron panel isn't necessary. Ferritin isn't normally part of an iron panel.)
• You will get a CBC as part of the test anyway; note CBC values of HCT, HGB, RBC
Also get before starting:
• LH
• FSH
• DHEA-S
• Cortisol
• Thyroid Panel
• Metabolic Panel
• Lipid Profile
There are thyroid problems that can mimic low Testosterone issues.
If you want a thyroid panel:
TSH
T3
T4
Normally only tested when there's a problem discovered with the above thyroid values:
Reverse T3
Free T3
Free T4
T3 Uptake/TBG
Thyroid Peroxidase (TPO) Antibodies
Thyroglobulin (Tg) Antibodies
"When do I get my blood draw?"
Generally, the day of your next dose before you take that dose. If you use gel, the morning of before applying. If a patch, the morning you change it before applying. If pellets, after day 7 post implant. If injecting once per week, 3 or 4 days after injection (why are you just injecting once per week anyway? Xyosted promotes a bad protocol). Testing on day 7 is only going to reiterate that you need Testosterone. Once-weekly dosing isn't TRT, it's just one big injection. Your Leydig cells didn't make Test once per week. Do diabetics take 350mg of insulin once per week? Tell your doctor to stop being stupid.
Order your own labs (Discounted Labs)
Order your own labs (Doctor Says)
Please be aware that 1) there are multiple schools of thought on ratio, 2) symptoms or absence of symptoms matters and this isn't just about numbers, and 3) "no research exists on this for men on TRT!" Actually, here's just one study on ratio that doesn't use the word ratio. "No studies exist" applies to injecting Testosterone more than once per week (yes, really).
Nelson Vergel commentary on ratio.
Free & Bioavailable Testosterone Calculator
Free Testosterone:
Not-SHBG bound Testosterone*:
Percentage of Total That Is Free: %
This calculator is shamelessly stolen from the ISSAM Calculator and re-implemented by me. It uses the Vermeulen equation to estimate free and bioavailable testosterone levels based on total testosterone, SHBG, and albumin concentrations. Reference "A Critical Evaluation of Simple Methods for the Estimation of Free Testosterone in Serum," Journal of Clinical Endocrinology & Metabolism, 1999.
Most guys don't get Albumin drawn, and the 4.3 is a presumed conservative average.
* SHBG bound Testosterone is used. We've known since 2005 that SHBG transports Testosterone into cells expressing megalin. [Source]
Visit roidplanner and chart your TRT / AAS cycle
Total doses available:
Volume per injection (mL):
Volume per injection (units on 1ml syringe):
Run-out date:
Days remaining:
Does dose divide evenly into the bottle
1. User Demographics
or
2. Activity Level
3. Goal
4. Special Conditions
Recommended Protein:
Range:
Per Meal (4 meals/day):
BMI:
Half Life
There are two types, Elimination and Terminal.
Elimination half life: The elimination half-life is the time required for the concentration of a drug in the bloodstream to decrease by half due to elimination processes, such as metabolism and excretion. This process begins immediately after the drug is administered (e.g., via injection) and continues throughout the drug’s presence in the body. The elimination half-life is a constant parameter that applies at any point during the elimination phase, not only after the peak concentration is reached (which for an injected ester in an oil base can be 24+ hours). Illustration.
Terminal Half-Life: The terminal half-life is the time it takes for the drug concentration in the bloodstream to decrease by half during the final phase of elimination after the drug has fully distributed throughout the body and elimination follows a consistent, first-order rate. It represents the tail end of the drug's presence in the body and is often shorter than the initial elimination phase because it's measured after the distribution and absorption phases have stabilized.
"94 to 97% of a drug will have been eliminated after 4 to 5 half-lives. Thus, it follows that after 4 to 5 half-lives, the plasma concentrations of a given drug will be below a clinically relevant concentration and thus will be considered eliminated." Source: https://www.ncbi.nlm.nih.gov/books/NBK554498/
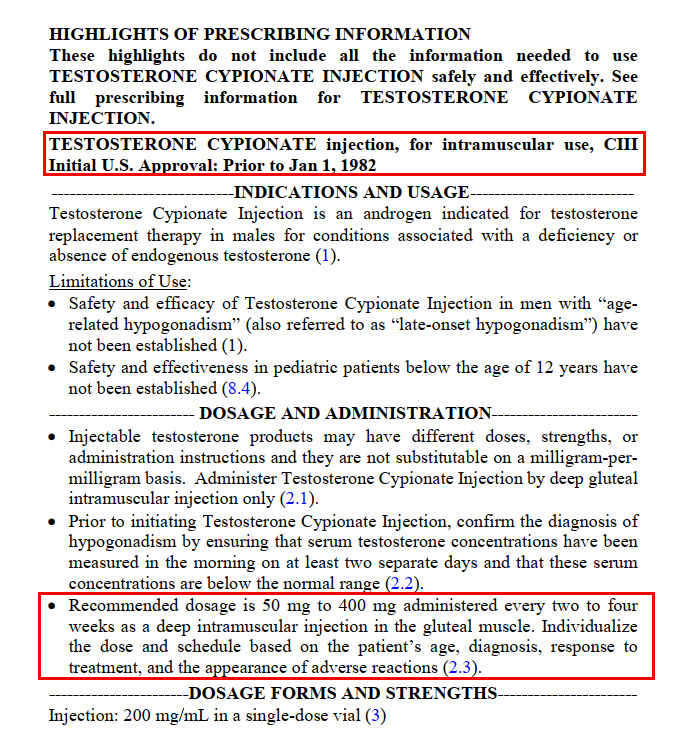
Why do some prescribers insist on 200mg every 14 days?
Here's your answer. It's from manufacturer data trialed in the 1970s and submitted to the FDA in the 1980s."50 to 400mg every 2 to 4 weeks" is pretty vague. Keep in mind that a "eugonadal" or "normal" level was 300ng/dL, just as it is now. So, yeah, 50mg every 4 weeks technically had some of the research subjects at a level of 300, I'm sure.
RIGHT CLICK, "OPEN IN NEW WINDOW" ON DESKTOP

"How quickly does a single injection of 200mg wear off?"
Comparative pharmacokinetics of Testosterone esters (see page 421 of PDF)
https://www.researchgate.net/publication/264848721_Pharmacology_of_testosterone_preparations/download
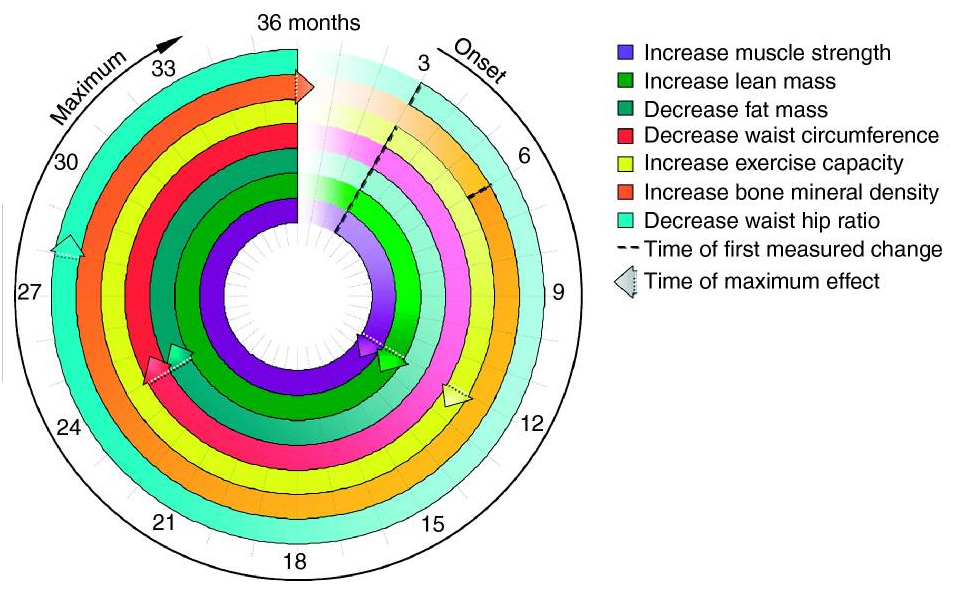
"How long does it take for symptom resolution?"
Onset of effects of testosterone treatment and time span until maximum effects are achieved
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3188848/
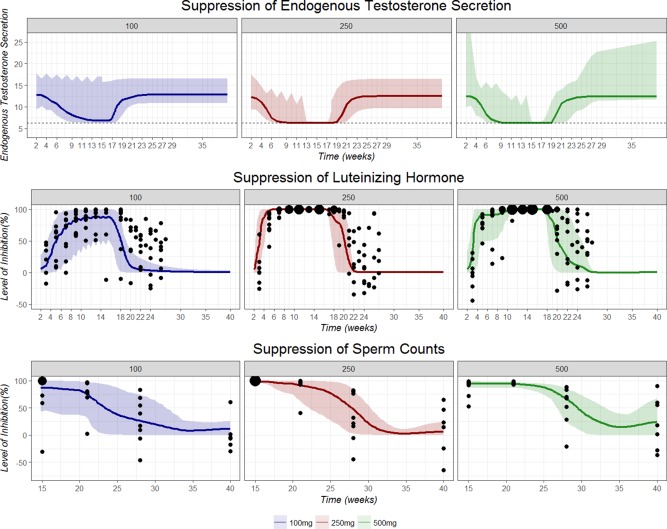
"How quickly does endogenous testosterone production shutdown occur?"
Population Pharmacokinetic/Pharmacodynamic Modeling of Depot Testosterone Cypionate in Healthy Male Subjects
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5915615/
"I heard that Testosterone Replacement Therapy causes cardiac issues. My doctor said it isn't safe."
Cardiovascular Safety of Testosterone-Replacement Therapy
https://pubmed.ncbi.nlm.nih.gov/37326322/
Estradiol
Estrogens, Male Reproduction and Beyond
https://www.ncbi.nlm.nih.gov/books/NBK278933/
hCG Guidance
Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6087849/
Blood pressure -- what can you take? (These are all metastudies)
Beetroot
https://pubmed.ncbi.nlm.nih.gov/29141968/
Garlic
https://pubmed.ncbi.nlm.nih.gov/26764326/
Citrulline
https://pubmed.ncbi.nlm.nih.gov/30788274/
Capsaicin, no significant effect
https://pubmed.ncbi.nlm.nih.gov/34676607/
Prostate cancer, long piece at Excelmale
https://www.excelmale.com/threads/is-testosterone-therapy-safe-after-prostate-cancer-treatment.34190/
Cabergoline FDA document (manage high Prolactin)
https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020664s011lbl.pdf
TRT Versus raising endogenous Test via SARMs, SERMs, Gonadotropins, and Aromatase Inhibitors
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7894643/
Carrier Oils
Nelson Vergel's Carrier Oil Discussion
A positive look at telemedicine provided TRT
Testosterone replacement therapy in the era of telemedicine
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8604198/
High Estradiol is associated with erectile dysfunction
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6987613/
https://www.nature.com/articles/s41598-020-69712-6
https://onlinelibrary.wiley.com/doi/abs/10.1111/and.14432
https://journals.lww.com/ajandrology/fulltext/2020/22060/estradiol_is_an_independent_risk_factor_for.14.aspx
Arimidex approval documents at the FDA
DIM (Diindolylmethane) seems to be an anti-androgen.
https://www.sciencedirect.com/science/article/pii/S1878535220302811
https://pubmed.ncbi.nlm.nih.gov/12665522/
Questions + Answers about Penile Injection Therapy for ED
https://www.excelmale.com/threads/27-questions-answers-about-trimix-penile-injection-therapy-for-ed.30907/
Fixing priapism after bimix / trimix overdose
"Some urologists have considered that oral administration of medications such as pseudoephedrine 60-120 mg orally or the asthma medication terbutaline 5-10 mg, followed by another 5-10 mg 15 minutes later can be used to treat ischemic priapism...
If after oral or intravenous medication use no detumescence occurs within 30 minutes, the next step is intracavernous vasoactive substances: metaraminol or agonists of E-adrenoceptors – phenylephrine, norepinephrine, ethylephrine and epinephrine... The literature data demonstrate that for all patients with ischemic priapism, resolution occurred in 81% of cases treated with epinephrine, 70% with metaraminol, 43% with norepinephrine, and 65% with phenylephrine."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3921718/
Low Testosterone and Anxiety: A Link Explained
https://www.sciencedaily.com/releases/2024/01/240122144432.htm
For women:
Plot your injectable Estradiol
A guide to prescribing testosterone for women in primary care
https://pmc.ncbi.nlm.nih.gov/articles/PMC7098532/
Testosterone Therapy in Women—What We Know in 2022
https://pmc.ncbi.nlm.nih.gov/articles/PMC9331845/
Low complication rates of testosterone and estradiol implants for androgen and estrogen replacement therapy in over 1 million procedures
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8165877/
Notable: The "established target postinsertion T ranges were 150–250 ng/dl for women... Because our study focused on complications from pellet therapy, some secondary reactions that occur with T use in women, such as body hair/facial hair, acne, and hair thinning, were not analyzed, representing another limitation of this study.
With the high continuation rate seen in our study, it is reasonable to hypothesize that the incidence of serious secondary reactions may be low. In addition, the results of studies conducted over the past 80 years regarding this therapy and its use on five continents have been uniformly positive with regard to the benefits versus the risks of T therapy."
Use of menopausal hormone therapy beyond age 65 years and its effects on women's health outcomes by types, routes, and doses
https://journals.lww.com/menopausejournal/fulltext/2024/05000/use_of_menopausal_hormone_therapy_beyond_age_65.3.aspx
Does Estrogen lower Testosterone? Yes:
Estrogen replacement therapy: effects on the endogenous androgen milieu
You were told by some random guy in a Facebook group who is 25 years behind on the science of Testosterone that "only Free Testosterone matters" because "SHBG is a suicide binder that 'binds up' almost all your Total Testosterone."
This is decades out of date.
Recent evidence has emerged, which challenges this traditional thinking and provides an insight into a possible alternative mechanism for androgen translocation across cell membranes. Megalin, a low-density lipoprotein endocytic receptor found in both male and female reproductive organs, has been shown to facilitate cellular entrance of sex steroids.
https://pubmed.ncbi.nlm.nih.gov/21322835/
SHBG is a transport protein that can transport androgens and estrogens into tissues that express megalin receptors.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4480437/
Contrary to the free hormone hypothesis, we demonstrate that megalin, an endocytic receptor in reproductive tissues, acts as a pathway for cellular uptake of biologically active androgens and estrogens bound to SHBG.
https://pubmed.ncbi.nlm.nih.gov/16143106/
Commonly referenced pages and communities
Dumped too much blood? The ferritin restoration protocol
Nelson Virgil's Excel Male forum
Peptide Calculator - how much BacWater do you add for a given dose
Steroid Calculator - plot your dose visually according to amount, ester, and injection frequency
Popular TRT telemedicine providers
United States
Often receive high reviews
Matrix
Defy Medical
Viking Alternative
Peter Uncaged
TRT Nation
No opinion expressed
Aspire Rejuevenation
Hone Health
Iamhrt
MeehanMD
Wellcore
Henry Meds
Evolve
RegenX
FountainTRT
Often receive negative reviews
Male Excel
Peak
Royal Medical
Marek Health
Canada
Science and Humans, formerly OnMen
GameDay Ontario
Waterloo Anti-aging
Sovereign Male
Canadian Men's Clinic
Jack Health
UK
Leger Clinic
Center for Men's Health
Optimale
Balance My Hormones
Prime Life Clinic
Alphagenix
Eden Clinic for Men
Manual
The Men’s Health Clinic