[Source of graphic]
What's the deal with Covid and iron and ferritin?
In order to understand fully what happens with iron dysregulation and why ferritin goes so high during a Covid infection, we need to review some basics.
We will focus on the effects of Covid with respect to ferritin and iron dysregulation. Covid infection is an extremely complex topic and this is NOT intended to cover every effect of the virus.
Up front: STOP taking iron during Covid. The 'why' will be explained later, but if you can't wait, click here, read the reason, and come back.
Is your Covid a mild case? Read this.
This summary was written when Delta was prominent. My links are mostly from when Beta was prominent. But now we appear to have a much milder variant, Omicron. It is possible that if you have a mild case of Omicron then the impact of taking iron is probably less dire. Similarly, if you were treated in the hospital with an anti-inflammatory like Dexamethasone, that would probably keep a lot of the below from happening. During Covid, you do have inflammation, so you'd be better off with heme iron if you supplement, since non-heme isn't even absorbed. Always talk to your physician (provided that your physician can explain what hepcidin is and how it works. If they can't, then they won't understand the issues with iron and Covid).
Let me repeat that -- if your doctor said it's "fine to take iron" in light of all of this research I have linked to below, ask them to explain how hepcidin works during Covid. They won't be able to. They. Are. Going. To. Make. You. SICKER.
1. Hemoglobin - a quick review
Hemoglobin (HGB) is the iron-containing oxygen-transport protein on Red Blood Cells (RBCs) that carries Oxygen to the body's tissues. A healthy individual has (Men: 13.5-18.0, Women: 12.5-16.0) grams of hemoglobin in every 100 mL of blood. Levels below these minimums are termed anemic. [Source]
2. Ferritin - a quick review
Ferritin is a protein that stores iron safely and is found mostly in tissue. [Source] (A little bit exists in serum. This amount in serum is reflective of tissue stores and is overflow.) [Source] About 80% of the body's ferritin is stored in the liver in cells called hepatocytes. Other key locations for ferritin are some of the macrophages in the spleen and bone cells. Lungs store some small amount of ferritin as well. [Source] (There are two types, L-ferritin and H-ferritin. In this article, we are only concerned with L-ferritin.)
On the other hand, serum iron is iron in the blood. When it's there, it's going to get put to use primarily in HGB and myoglobin. [Source] Serum iron varies in everyone from day to day -- ferritin doesn't normally change that fast unless you lose blood (such as through donation or a heavy, lengthy period). [Donation] [Periods]
Iron is transported through the blood by transferrin. On an iron panel, you will see a Transferrin Saturation Percentage (TSat%). That is a good indicator of your serum iron. In normal people, it's between 20 and 50. Lower is a sign of iron deficiency. Higher is a sign you just had iron too close to your blood draw, or you have a disorder such as hemochromatosis.
For our purposes, it's best to think of serum iron and ferritin as opposites. Iron is either in the blood, or it's stored in tissue. That's not 100% accurate, but it's helpful to think of it this way for our purposes here.
You can't have a piece of cake in front of you after eating it. It's one or the other. Similarly, iron is either in blood or it's in tissue as ferritin.
There is evidence that in women, a minimum level of 51 is where the body attempts to correct for low ferritin. No similar research exists for men that I am aware of, but for now that's a reasonable minimum value for deficiency (not 5, not 15, not 20!). [Source] One doctor recommends a sustained minimum level of 100 to resolve common symptoms of iron deficiency without anemia such as RLS. [Source] The Hartigan Iron Protocol recommends 125+ sustained for 6 months at least. A common maximum given in lab ranges is 400.
THERE ARE TWO WAYS TO BUILD FERRITIN:
1. take iron, the body uses it to maintain a healthy HGB, and the body stores the extra iron as ferritin (preferred method).
or
2. elevate hepcidin, trapping the iron from recycled Red Blood Cells in tissue, which is stored as ferritin, which includes ferritin (this is NOT a preferred method because it can lower RBCs and hemoglobin).
This piece will be discussing method 2 -- it's what inflammation does.
3. Hepcidin - a quick review
Since its purpose was discovered in 2001, the peptide hormone hepcidin has been identified as the principal regulator of iron availability in the body. [Source] [Source]
Hepcidin has TWO main functions:
1a. Protecting us during infections by depriving pathogens of iron, a key food source
1b. Directly entering a cell and acting as an anti-microbial
2. Protecting us from iron overload
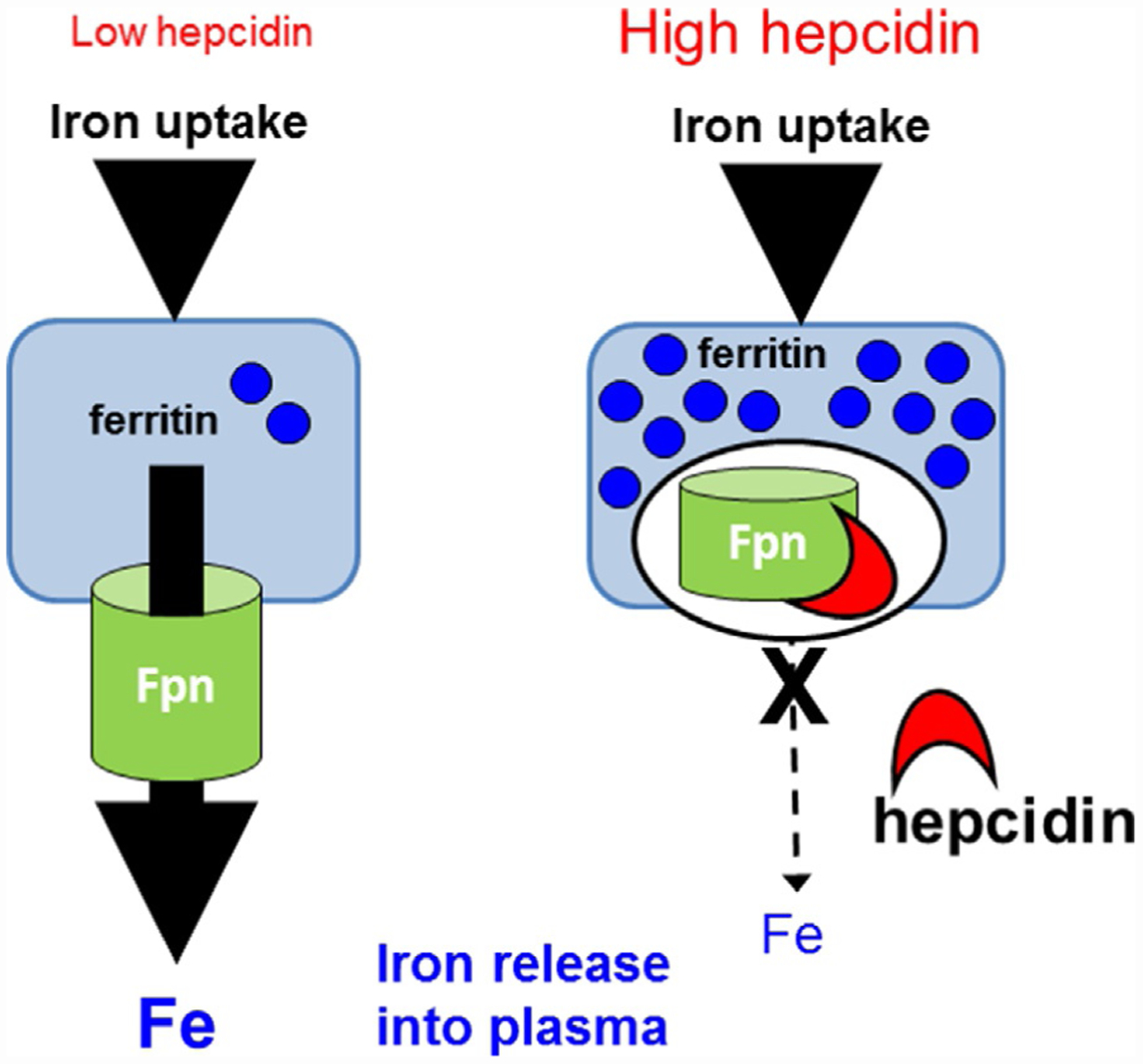
It does the same group of things whether you're sick with a virus or bacterial infection, or whether you foolishly ingested an entire bottle of iron pills: it will block iron absorption in the intestine while simultaneously preventing iron transport out of liver and spleen cells (it does both no matter what. It is never one or the other). [Source]
Specifically, hepcidin, when it's high:
1. traps iron in cells of the small intestine (duodenal enterocytes). [Source] "This iron would be eventually lost [in feces] through the routine sloughing of enterocytes, which turn over approximately every 3 days in humans." [Source]
2. blocks iron release by liver cells (hepatocytes) by binding to and degrading ferroportin.
3. traps ("sequesters") iron in macrophages of the liver, spleen, and bone marrow also by binding to and degrading ferroportin.
Ferroportin is the cellular "drain" that lets iron out of cells. This protein serves as an iron exporter in cells that recycle iron from senescent [aging] red blood cells." [Source] So hepcidin essentially acts like a drain plug. 80% of the body's ferritin is the iron in the liver's cells alone. [Source] [Source]
RBCs flow into liver and spleen and the iron is recovered as the cells are retired. Unlike iron you take in a pill or food, this recycled RBC iron never, ever sees binding to transferrin.
In all of these cases, trapped iron cannot enter the blood when hepcidin is high. Elevated hepcidin therefore means that this iron temporarily has nowhere to go, so hepcidin is "effectively shunting cellular iron into ferritin stores and preventing its absorption into the blood." [Source] You make, and retire, 200 billion RBCs every day. Hepcidin will restrict iron availability for erythropoiesis [making RBCs], so making RBCs will be throttled back. [Source] HGB will fall from that, as well as from hepcidin restricting iron from serum. Nonetheless, that iron from recycled RBCs is going to pile up fast if it stays trapped. [Source]
Put it all together: you now have RBCs falling, HGB falling, and ferritin going up.
A comprehensive discussion of what regulates hepcidin may be found here: the major regulators of hepcidin blood levels are iron status and consumption, anemia, hypoxia, and inflammation.
You need hepcidin to build ferritin. It's not always the bad guy: "Serum ferritin was shown to be the most important correlate of serum hepcidin concentration. A positive regression coefficient was found, indicating that increased serum ferritin concentration is associated with increased serum hepcidin concentration, which has consistently been reported before." [Source]
A brief note. Although ferritin is going up, with RBCs and HGB falling, the only people who would benefit are people with too many RBCs like polycythemia vera or erythrocytosis. They need higher ferritin, but unlike most people, they also need their RBCs reduced.
4. Inflammation - A quick review
"Inflammation is a biological response of the immune system that can be triggered by a variety of factors, including pathogens, damaged cells and toxic compounds. Both infectious and non-infectious agents and cell damage activate inflammatory cells and trigger inflammatory signaling pathways." [Source]
"Almost all inflammation markers and iron indicators correlate significantly with hepcidin." [Source] Interleukin 6 (IL-6) exerts the strongest effect, but a multitude of inflammatory markers can elevate hepcidin.
"Although IL-6 is known to induce hepcidin expression in inflammatory conditions, a key hepcidin upregulatory pathway [via the STAT3 gene] can be activated by a plethora of other cytokines and growth factors." [Source]
"The increase in the hepcidin level in response to pathogen infection is not equal across every infection, for example, in patients with AIDS/HIV infection, hepcidin is increased, but not in hepatitis B and C. It is thought that hepcidin-induced hypoferremia is determined by the type of pathogen, site of infection and typical immune response. During inflammation and infection, the activated macrophages will unleash cytokine networks, which contain IL-6. The quantity of IL-6 induced by hepcidin secretion depends on the severity of the inflammation. In contrast, when the inflammation is resolved, the erythroferrone precursor (ERFE) will facilitate hepcidin down-regulation and will accelerate the recovery process of the organism from iron disorders during the inflammatory process." [Source]
Simply put, when inflammation subsides, hepcidin drops, ferroportin is able to export iron from cells again, and ferritin stores are available to the body. The "iron drain plugs" have been removed from the cells. All that iron stored as ferritin is ready to be put by the body into serum. Hello, massive ferritin drop.
5. Ferritin rising from inflammation - A quick review
Earlier we said that there are two ways to build ferritin:
1. Taking iron with vitamins C and D to keep hepcidin low. The body uses the iron to maintain a healthy HGB, and the body stores the extra iron as ferritin (preferred method). This builds HGB and stores the extra iron you took as a pill or infusion as ferritin. This is the basis of The Hartigan Iron Protocol. Builds HGB first, ferritin second.
2a. Raising hepcidin via massive doses of non-heme iron pills (heme iron uses a different absorption path). This elevates hepcidin, trapping the iron from recycled Red Blood Cells in tissue, which is stored as ferritin (this is NOT a preferred method). This lowers HGB and stores endogenous iron from your red cells as ferritin. This uses the BMP/SMAD pathway. Builds ferritin first, lowers HGB. Can make you anemic. Click [Source] and scroll to "3. Regulation of hepcidin expression."
2b. Raising hepcidin via inflammation. This also elevates hepcidin, trapping the iron from recycled Red Blood Cells in tissue, which is stored as ferritin (this is NOT a preferred method). This lowers HGB and stores endogenous iron from your red cells as ferritin. This uses the Interleukin-6 pathway. Also builds ferritin first, lowers HGB. Can make you anemic. Click [Source] and scroll to "4. Hepcidin regulation by inflammation."
BOTH PATHS 1 AND 2 MAKE THE SAME REAL, ACTUAL FERRITIN.
You can change a light bulb using a step ladder or standing on a milk crate but you wouldn't say step ladders are the same as milk crates. On the flip side of that coin, neither method changes the new light bulb you're holding in your hand. It's still the same new bulb.
A ferritin blood test measures ferritin. Ferritin made via one route is molecularly identical to ferritin made via the other route. [Source]
You may be familiar with the term "false ferritin." False ferritin refers not to the ferritin itself but how it is transient and will not be sustained.
"False Ferritin" explained using a money metaphor
Here are two possible ways to get $50,000:
• Raising ferritin with inflammation is like robbing a bank. You got it FAST. It's still real, actual money. But those sirens in the distance mean it's not going to be around for long. It's "false riches."
• Raising ferritin with an iron protocol is like giving money to a broker to invest. It's real, actual money that you're building slowly and sensibly.
Recall the explanation above that when hepcidin is high, as a normal function of what it does, iron is restricted from serum. HGB falls. The increase in the hepcidin level in response to pathogen infection is not equal across every infection. The cytokine response to Covid (and many severe influenzas and other conditions) is massive.
To say it again simply, if hepcidin is high for a sustained period of time, you'll become anemic and your ferritin can actually go up -- mainly in the spleen and liver, where RBCs are retiring.
When you get better, inflammation subsides, hepcidin drops, and your body uses the ferritin to rebuild HGB. That, of course, is how it's supposed to work. Your body seeks an optimal HGB (highly individualized) and uses ferritin to do it. If you had a high HGB, such as 17, your body wouldn't take from ferritin stores.
I want to repeat that for emphasis. If you had a high hemoglobin, such as 17, your body would NOT take from ferritin stores. However ferritin got to be high, it can stay high if hemoglobin is high. (This is rare but happens to some males after they recover.) This fact will come into play later.
A quick side note. Some people talk about ferritin solely in terms of inflammation. If you read and understood everything up to this point, you understand why certain "movements" saying ferritin is bad are nonsense.
Hepcidin is an acute phase reactant, but it is raised via a few different methods -- not just inflammation. FERRITIN IS NOT BAD OR TOXIC. The iron administration pathway is distinctly different from the inflammation pathway.
6. Covid and ferritin and iron
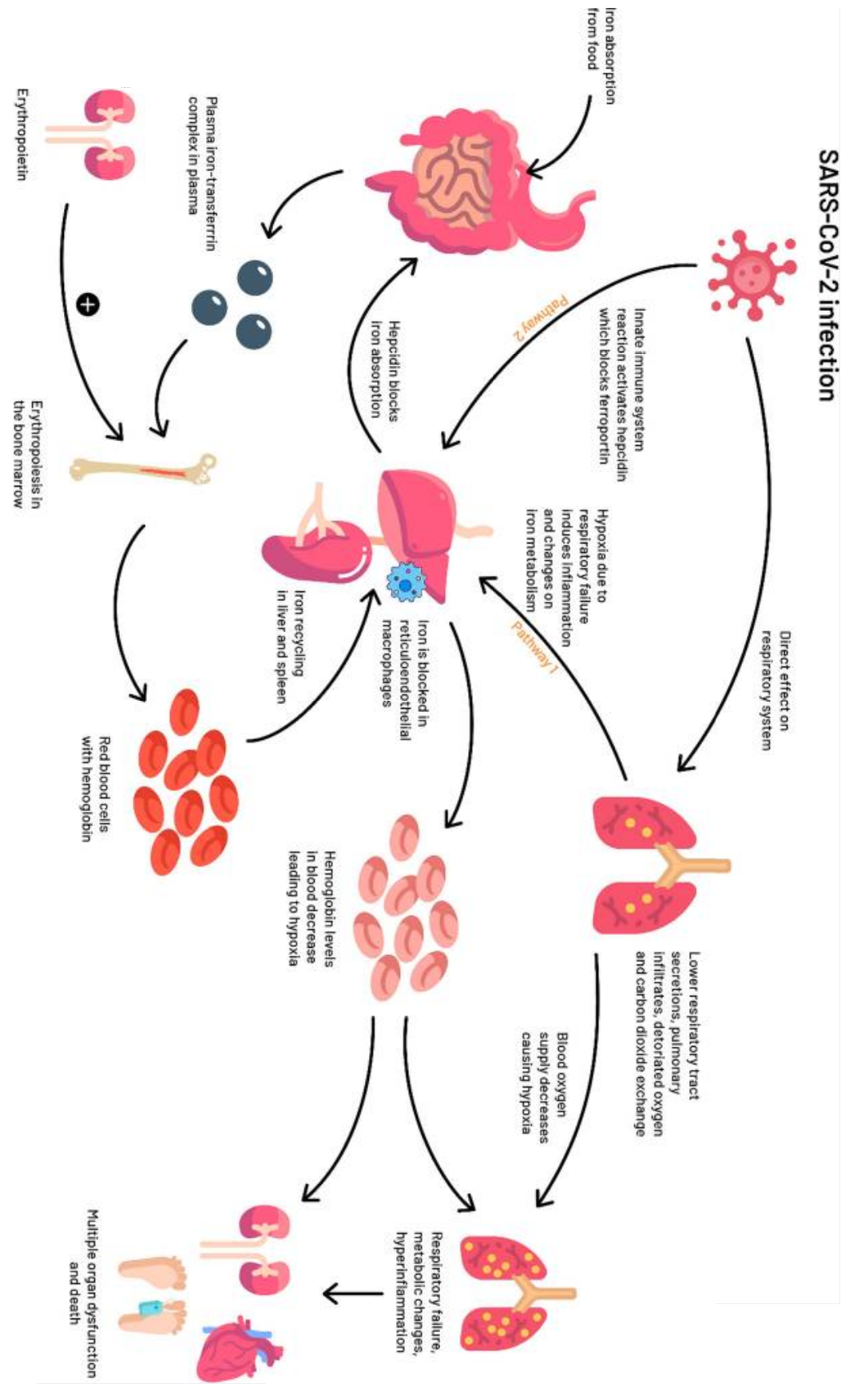
Let's put everything we've read so far together. (If you understood everything up top, you can skip down to the graphic). The following is excerpted from this study. It distills in original study language everything that was explained above:
The innate immune system orchestrates control over iron metabolism as a response to viral infections. For viral replication, enhanced cellular metabolism and optimal iron levels within host cells are necessary. Therefore, the innate immune system will react by decreasing the bioavailability of iron to limit the replication of the virus during the acute phase of infection. In these conditions, through interleukin-6 and Toll-like-receptor-4 dependent pathways, the levels of the liver-derived iron hormone hepcidin, the master regulator of iron homeostasis, could increase and block the activity of the transporter ferroportin which carries iron out of the cells, and therefore decrease the amount of iron absorbed from the diet, causing cellular sequestration of iron (i.e., principally in hepatocytes, enterocytes, and macrophages). Increased intracellular iron sequestration will lead to an upregulation of cytosolic ferritin, which sequesters and stores iron to prevent iron-mediated free radical damage. The increased retention and storage of iron within ferritin in macrophages contribute[s] to the characteristic fall in serum iron concentrations and an increase in serum ferritin concentrations as observed in an acute phase response. The net result will be a diminished iron availability for erythropoiesis and as a result further aggravation of anemia.
TAP TO OPEN LARGER ON MOBILE, OR
RIGHT CLICK, "OPEN IN NEW WINDOW" ON DESKTOP
Again, when ferritin rises because hepcidin is high, whether by taking handfulls of iron pills or inflammation, the high ferritin comes at the expense of lowering hemoglobin. Let's dive into some detail.
It is known that Covid precipitously raises IL-6 (as well as other inflammatory cytokines). [Source] The cytokine response in itself can be fatal in some people which is why corticosteroid drugs like Dexamethasone are given. Yes, you are reading this right. A drug that weakens the immune system is given because the inflammatory cytokine response during Covid can kill you.
Multiple studies specifically identified higher levels of IL‐6 among patients with more severe (complicated) disease. Some studies are showing the highest ferritin levels among the deceased, but there doesn't seem to be agreement on that. [Source] [Source]
... Viral attack via reduced hemoglobin
COVID-19 patients tend to present decreased hemoglobin levels indicating the presence of anemia, and pathologically increased levels of ferritin. [Source] As we would expect from what we read earlier about prolonged elevated hepcidin. Just how high could ferritin go? "Based on findings from 54 observational studies, including 24,262 COVID-19 patients, pooled mean ferritin level in COVID-19 patients was 777.33 ng/mL." [Source]
When we talk about HGB and Covid, we need to remember that selection bias is at work. Measuring HGB is generally only done in the hospital context. So we have to consider that although Covid lowers HGB, the people who were sickest were the ones who presented to the ER.
Hemoglobin levels go lower by comorbidities, in order: being over 55, cardiovascular disease, diabetes, and hypertension. [Source] One small sample size study result found a 38% drop in HGB during hospital stay. [Source] At the start of the pandemic, there was a lot of discussion "largely relayed in the media and social networks" about the causes of O2 saturation drop. It is therefore important to note that it has been shown that Covid does not alter O2 binding to HGB. [Source] The hypoxia is chiefly from low HGB.
Patients with Acute Respiratory Distress Syndrome (ARDS) as can happen with Covid have elevated levels of cell-free hemoglobin in the air space. [Source] Nitric oxide (NO) secretion usually compensates for hypoxia inducing vasodilation, but circulating cell-free hemoglobin (hemoglobin outside of the red blood cells) would impair NO bioavailability. [Source]
... Viral attack via hemolysis (red blood cell destruction)
"A viral interaction with [the] hemoglobin molecule, through ACE2, CD147, CD26 and other receptors located on erythrocytes and/or blood cell precursors, has been highlighted. ... [I]t has been argued that hemoglobinopathy would derive from viral endocytosis, through a linkage between spike proteins and cell receptors. ... SARS-CoV-2 would consequently induce hemolysis [destruction of RBCs] and/or form a complex with the released heme, generating ... dysfunctional hemoglobin, with reduced oxygen and CO2 transport. [Source]
"Red cell distribution width (RDW) represents a reliable marker of myelodysplasias, being higher when immature cells are produced. COVID-19 literature repeatedly highlights a generally increased RDW, which is significantly higher (>14.5%) in deceased or critical patients." [Source]
Same source: "thalassemic patients, ... seem to exhibit a good prognosis, due to the reduction of hemoglobin beta-chains (potential virus’ target); ... thalassemia-associated low hepcidin secretion may represent another protective mechanism."
Same source: "Together with the previously reported molecules, the GRP78 receptor has been considered another SARS-CoV-2 entryfacilitator [and is] also located in bone marrow stem cells. ... this additional receptor would facilitate anti-hemoglobin viral action on hematopoietic stem cells ... Of interest, free circulating heme typically injuries endothelial cells, as well as ferritin overdeposit may contribute to vascular wall remodeling... hepcidin/ferroportin dysregulated interaction may create pulmonary artery hypertension. ... hyperferritinemia [also] progressively [worsens] alveolar-capillary/cell membrane integrity/permeability."
... Viral damage from free (unbound) circulating iron
In iron overload conditions, unregulated iron entry into the plasma overwhelms the carrying capacity of transferrin, resulting in non-transferrin-bound iron (NTBI), a redox-active, toxic form of iron. [Source] (By the way, when TSat% gets too high for a sustained period of time and you aren't taking iron, that is what is happening. High circulating NTBI.)
Covid causes greater ferritin deposit in the lungs, which causes high levels of pulmonary oxidative stress. [Source] [Source] In fact, any extremely high level of ferritin causes overflow deposit of ferritin in pulmonary tissue. [Source] (Remember, we're talking a mean ferritin of 777 here. By "high" we do not mean 400.)
Hyperferritinemia in Covid is a driver of worsening disease as well as a reflection of an out-of-control cytokine response, mainly IL-6.
... Covid is a hepcidin mimetic
We've already described how hepcidin enters cells to fight pathogens directly, and (by degrading ferroportin) essentially acts as an iron drain plug in the cell, trapping iron from recycled RBCs, storing it as ferritin.
Hepcidin evolved so long ago that it is literally found in all vertebrates. Hepcidin in fish works in mice. Mouse hepcidin works in human cells in vitro (test tube). A biological agent doesn't have to be an exact, 100% precise fit to work.
The TM-CT junction of the spike protein appears to have the potential to act as hepcidin acts. Even if we were able to suppress hepcidin, say with an anticoagulant that suppresses hepcidin, we still may have the virus itself acting to raise ferritin to pathological levels. At the time this similarity was noted, it was unknown whether the virus acts as hepcidin once it has entered the cell. [Source]
7. Further Reading
Covid: is it time to re-design iron supplementation programs? [Source]
Raising ferritin AFTER Covid treats a case of Long Covid [Source]
Covid and the B vitamins. [Source]
Did you see a reliable story or study that you think I should include? Send me a message on FB and let me know.
8. Common Questions
Should you continue dosing iron during your illness?
This is a resounding NO. As we know:
1. non-heme iron simply isn't getting absorbed when hepcidin is high
2a. heme iron (which bypasses hepcidin) enters the blood and fills cells (because of hepcidin, there's no ferroportin to let it out of cells) which adds to existing hyperferritinemia from the virus
2b.
heme iron also increases serum transferrin level [source] and transferrin level correlates with clot risk and worse outcome [source]
3. any absorbed iron that enters the blood (not sequestered) feeds viruses
Simply put -- taking iron while sick with a virus as powerful as Covid is not doing you any good. In fact, studies mention using iron chelators such as Deferoxamine to decrease ferritin levels. It can really be that bad. Serum iron overflow affecting organs such as the lungs during Covid is a very real risk.
"I am a contrarian who doesn't want to read ANY of the links in this. I just want to disagree and say taking iron with Covid is fine."
Here are two quick summaries:
When can you resume dosing iron?
When inflammation subsides. This could be all of your WBCs within normal ranges on a CBC, or 48 hours fever-free. If you can crush inflammation with Dexamethasone or a similar drug, you arguably could resume your iron earlier.
I want to remind the reader that some people have suddenly felt better after a few days only to see Covid symptoms really surge back. So if you think your case only lasted 3 or 4 days, you will want to be sure you're really better!
"But WBCs only mean infection, not inflammation!"
Infection with what? Covid? Guess what. Infection with Covid causes inflammation. A CBC isn't telling you iron is safe. A CBC is telling you whether Covid has subsided or not. [Source] Since hyperferritinemia is driven by Interleukin 6 (see above), then an IL-6 blood test would be the gold standard here, but I don't think a doc will order that for you.
But my ferritin dropped!
After your illness? Yes, that's expected. During your illness? Not unless you were given an anti-inflammatory drug like Dexamethasone.
Will my new high ferritin level drop after I recover?
There's a good chance it will, yes. Covid built up ferritin at the expense of HGB, which dropped. When you are better and the inflammation subsides, the body will use the ferritin to put the stored iron into HGB. Under rare cirumstances, some males with a high HGB, like 17 or higher, may find that their ferritin doesn't go down (think of these guys as the bank robbers who stole the $50,000 and got away with it). The rate of ferritin fall depends on your HGB. Covid's lowering people's HGB so let's assume that ferritin's going to fall fast for many. For those who are stuck with the high ferritin, it can be managed with phlebotomy or, as mentioned earlier, chelators.
Explain the hair loss (alopecia)?
Anogen or Telogen Effluvium. "In a normal healthy person's scalp, about 85% of the hair follicles are actively growing hair (anagen hair) and about 15% are resting hair (telogen hair)." [Source]
Anagen Effluvium refers to hair shedding that arises during the anagen or growth stage of the hair cycle. [Source] Can result from inflammation.
Telogen Effluvium is hair shedding that arises during the telogen or resting stage of the hair cycle. [Source] Can result from psychological stress or iron deficiency. Telogen effluvium is known to happen in conjunction with low ferritin. [Source]
We know low ferritin causes hair loss anyway. [Source] We can only assume that rapid ferritin drops will precipitate more pronounced Telogen Effluvium.
You didn't cover [some effect of Covid]?
I really don't have the time to do an in-depth piece. I wanted to keep this relegated to ferritin and serum iron.
Who are you?
Long story short, I have been reading intensively about hepcidin for a really long time, and so I easily understood the issues discussed in the research. I hope I have communicated things clearly for the average person. I am not a doctor; my clinical knowledge comes from training to the EMT-Intermediate/99 level (retired as of 2007). I am a HIPAA compliance officer at a hospital.
Dude you kept it under 4,000 words!?
Yeah I'm kinda proud of myself for that to be honest.
{kind=link}